← Platform Overview
Senovia Biosciences · Scientific Brief · SNV-301
Metabolic Psychiatry: Complete Remissions in Treatment-Resistant Patients via Bioenergetic Restoration
A century of clinical observation. Documented remissions where pharmacotherapy failed.
Never pharmaceuticalized.
Abstract
Emerging human evidence demonstrates that metabolic state correction produces complete
psychiatric remissions in patients who have failed standard pharmacotherapy. Across independent
case series and controlled inpatient studies, ketogenic metabolic therapy (KMT) has achieved
PANSS reductions of 46% in refractory psychotic illness (p<0.001), complete PHQ-9
remission in treatment-resistant depression, and transdiagnostic symptom resolution across
PTSD, ADHD, and binge-eating disorder. These effects occur in patients classified as
treatment-resistant by conventional criteria. The mechanistic basis centers on correction of
cerebral glucose hypometabolism, mitochondrial dysfunction, and neuroinflammation, pathologies
shared across psychiatric diagnostic categories. SNV-301 aims to deliver pharmaceutical-grade
ketosis as an oral, titratable therapeutic, converting dietary observation into a registrational
drug program.
46%
PANSS reduction in
refractory inpatients
Danan 2022
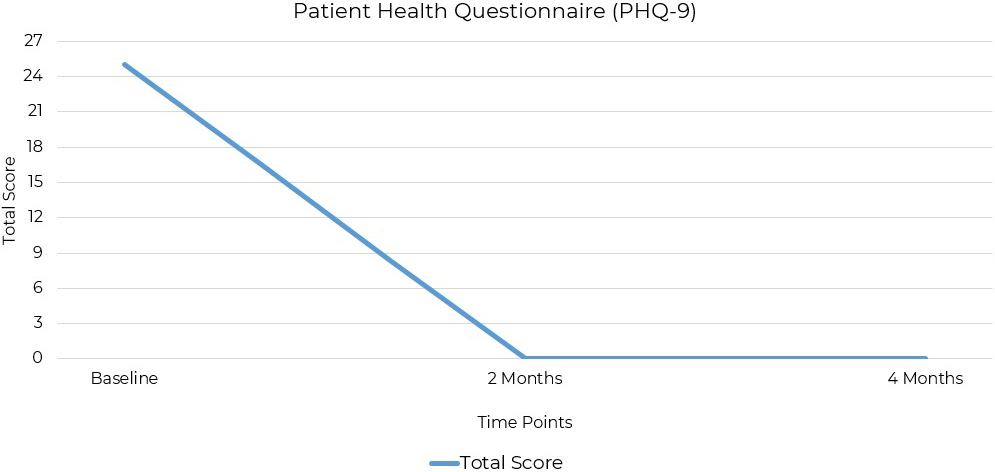
PHQ-9: 0
Complete remission
in lifelong TRD
PMID 40083888
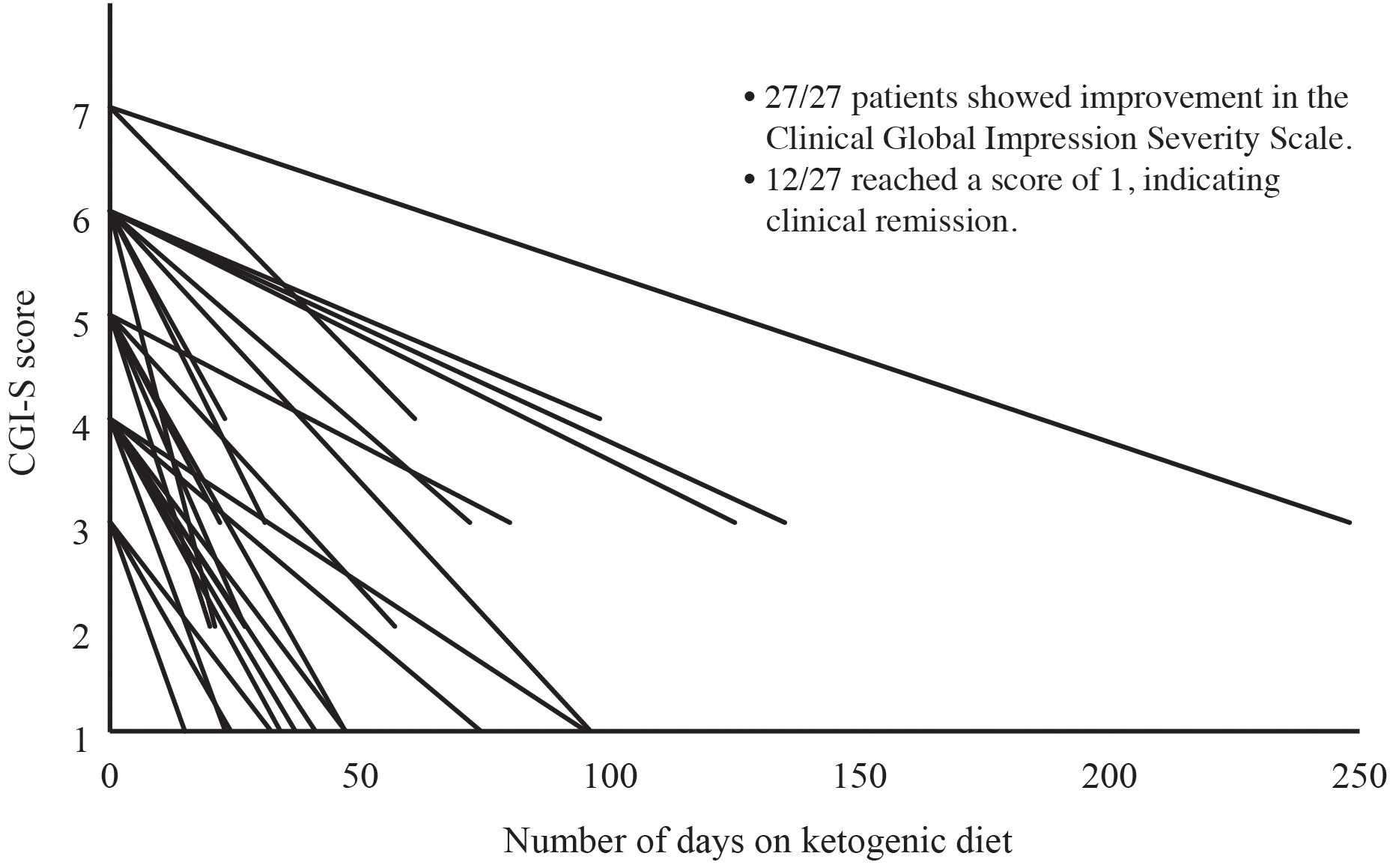
27/27
Inpatients improved
on CGI-S
Danan 2022
505(b)(2)
Regulatory pathway
for known substrates
Evidence Context
Human evidence: Multiple independent case series and controlled inpatient studies documenting complete
remissions in treatment-resistant patients. No completed RCTs of exogenous ketone therapy for
psychiatric indications. Mechanistic rationale supported by extensive preclinical and human
neuroimaging data. Pipeline status: IND-enabling.
1. The Metabolic Basis of Psychiatric Illness
The ketogenic diet was first applied to psychiatric conditions in the 1920s, alongside its use
in epilepsy. Mood stabilization, psychosis attenuation, and reduced agitation were documented
before the first antipsychotic existed. A century later, the field is converging on a unifying
explanation: major psychiatric disorders share metabolic pathology.
Glucose hypometabolism has been demonstrated on PET imaging in schizophrenia, bipolar disorder,
and major depression. Insulin resistance occurs in psychiatric populations at 2-3x the rate
of age-matched controls. Mitochondrial dysfunction, indexed by lactate elevation and reduced
ATP production, has been identified across diagnostic categories. The brain consumes 20%
of total body energy at 2% of body mass. When that energy supply fails, neural circuits fail.
The Insight
If psychiatric symptoms emerge downstream of metabolic failure, then correcting the metabolic
state should produce symptom resolution independent of neurotransmitter manipulation. That
is exactly what the clinical data show.
The gap between observation and therapy has persisted because dietary ketosis cannot be patented,
prescribed, or titrated. Compliance rates for the ketogenic diet in psychiatric populations are
low, and the intervention is incompatible with controlled clinical trial design. SNV-301 resolves
this by delivering pharmaceutical-grade ketosis in an oral, titratable format.
2. Human Clinical Evidence: Remissions in Treatment-Resistant Patients
The following table summarizes published human clinical data. Each study involved patients
classified as treatment-resistant by conventional pharmacological criteria. Effect sizes are
reported as published; all citations link to indexed, peer-reviewed publications.
| Condition |
Population |
Outcome |
Effect |
Source |
Refractory psychiatric illness
(bipolar, schizoaffective) |
31 inpatients, 6-week KD |
PANSS 91.4 → 49.3 |
46% reduction
p<0.001 |
Danan 2022 |
| Treatment-resistant MDD |
47yo female, lifelong TRD |
PHQ-9: 25 → 0 at 8 weeks |
Complete remission |
PMID 40083888 |
| Schizoaffective disorder |
17yo female, severe psychosis |
Cessation of hallucinations
and suicidal ideation |
Full remission @ 6 wk |
Laurent 2025 |
| Schizoaffective disorder |
32yo female, chronic |
Full remission; psychiatric
medication discontinued |
Deprescription |
Laurent 2025 |
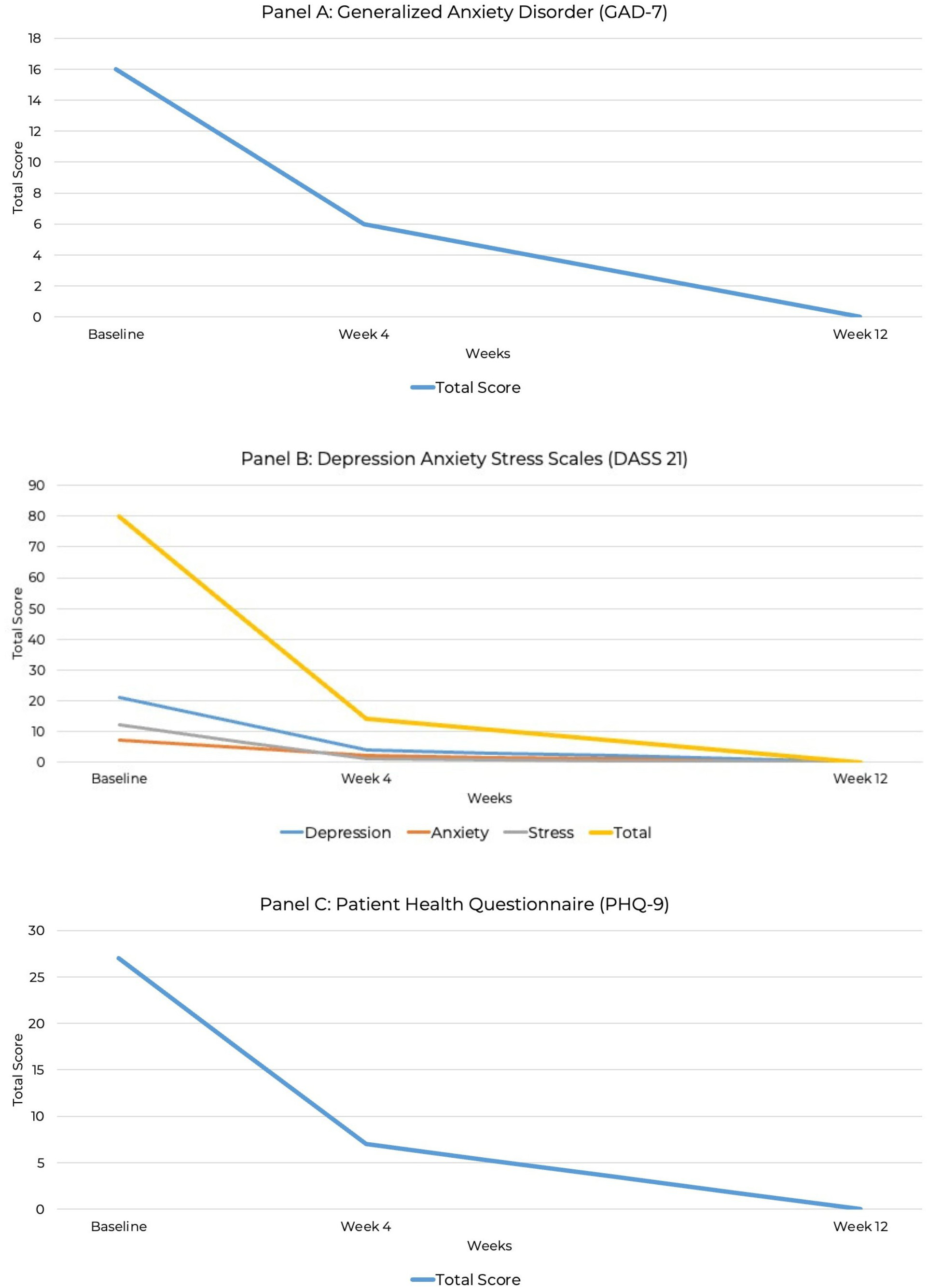
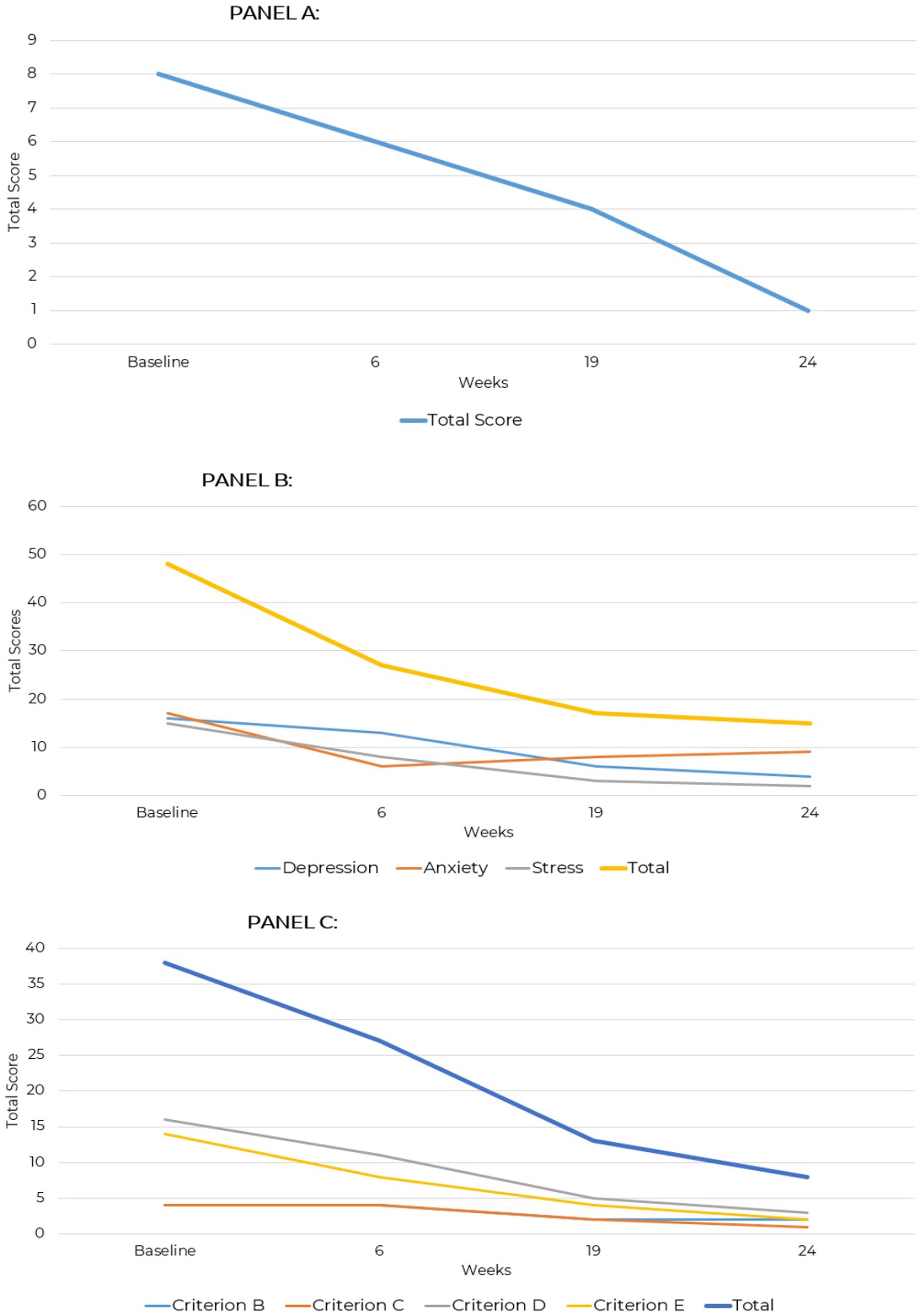
Transdiagnostic
(PTSD, ADHD, binge-eating) |
Adult, all prior Tx failed |
PHQ-9, GAD-7, DASS-21
all reduced to 0 by week 12 |
All scales → 0 |
PMID 40626225 |
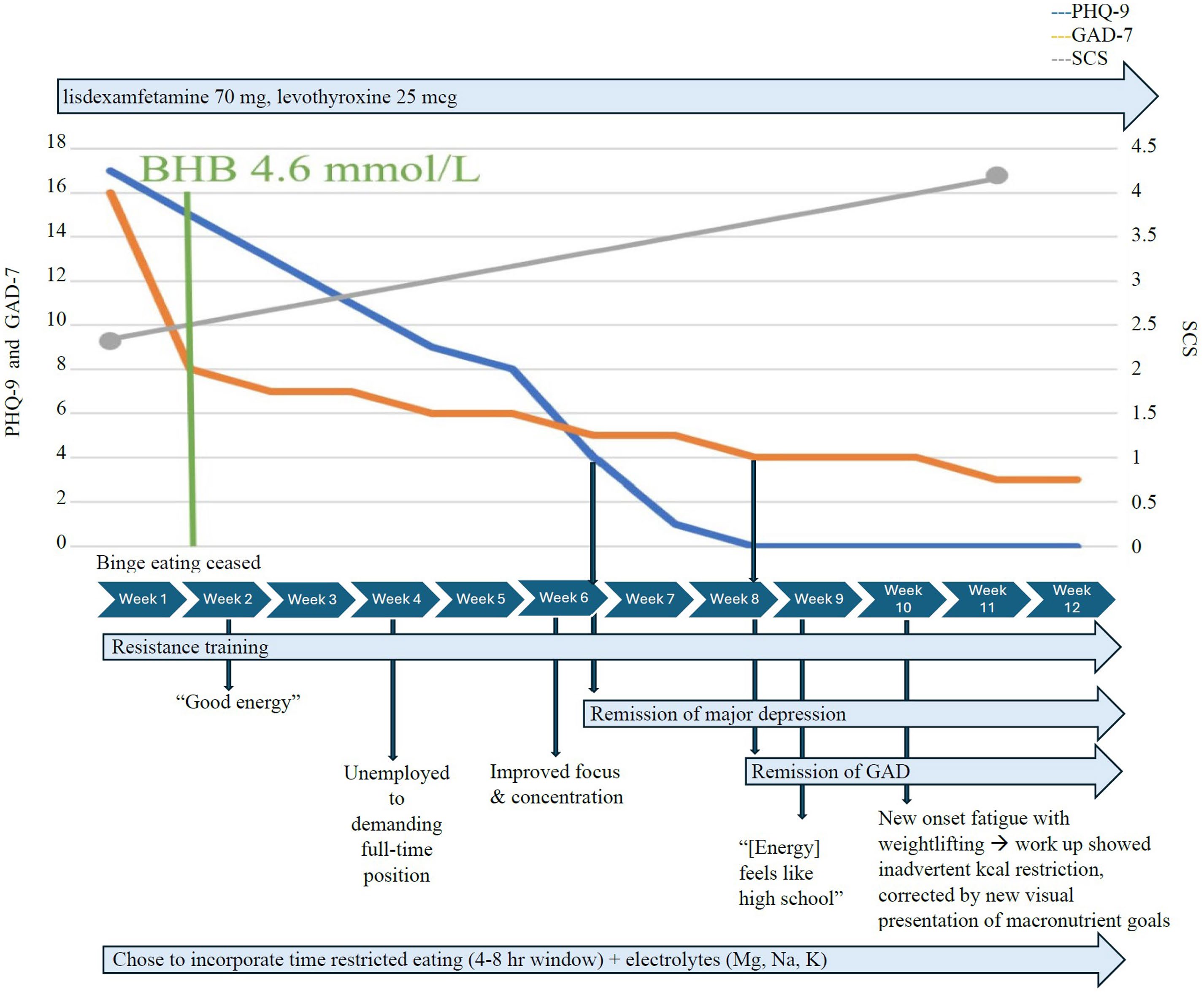
| MDD + GAD |
3-patient case series |
Complete remission of MDD
and generalized anxiety |
Remission @ 7-12 wk |
Needham 2024 |
| OCD + ulcerative colitis |
37yo female |
Y-BOCS 0, FOCI 0,
UC clinical remission |
Dual remission @ 12 wk |
PMID 40248603 |
| Bipolar, treatment-resistant |
Adult, failed ketamine |
KMT + ketamine →
sustained remission |
Failed ketamine; responded to KMT |
PMID 39188977 |
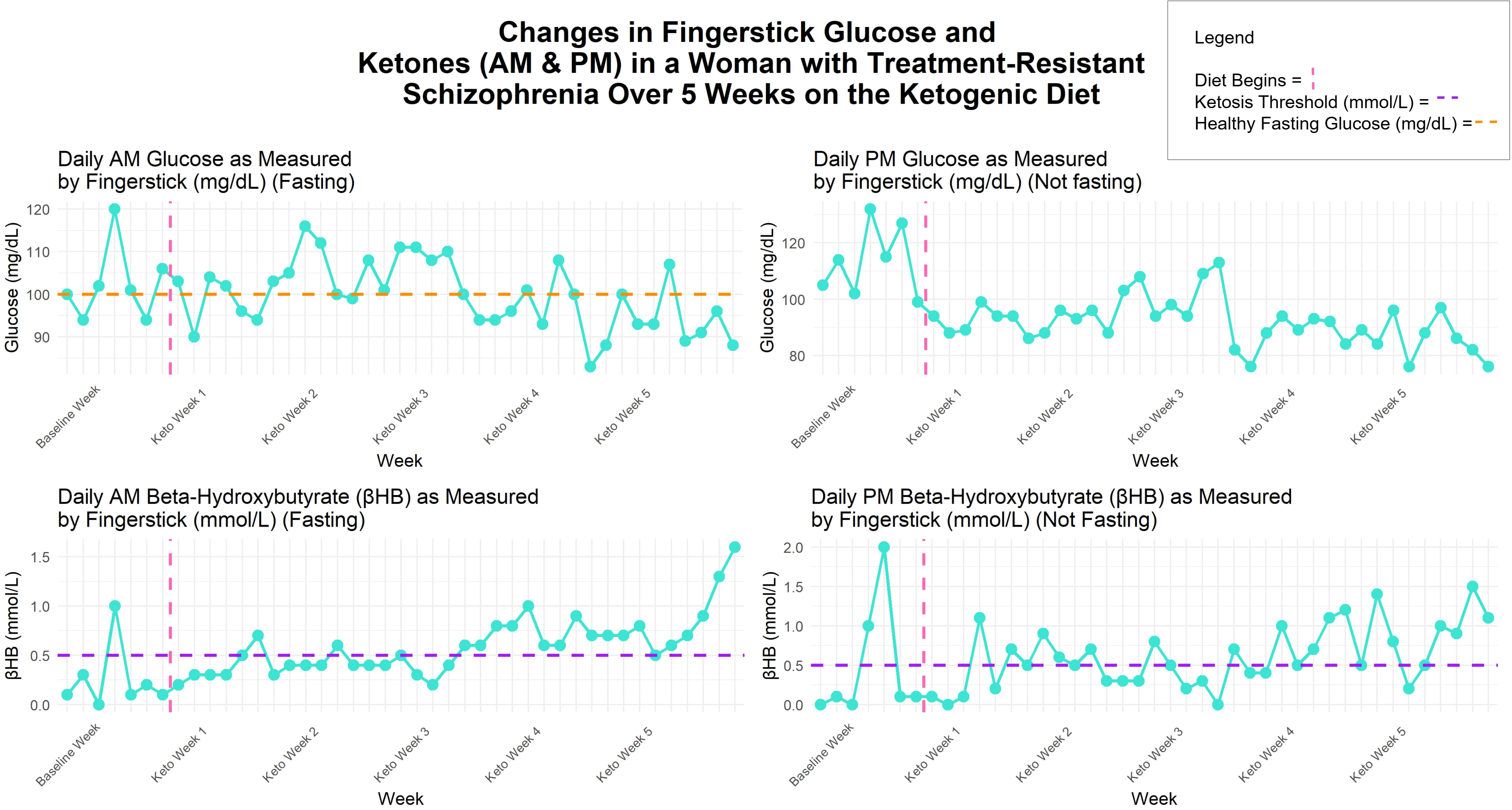
| Treatment-resistant schizophrenia |
48yo female, 5-week inpatient |
HOMA-IR ↓69%, CRP ↓61%,
extrapyramidal symptoms ↓80% |
Metabolic normalization |
PMID 41356674 |
| Severe anorexia nervosa |
Enduring AN, KD + ketamine |
Weight restoration,
symptom cessation |
Complete remission |
PMID 32848935 |
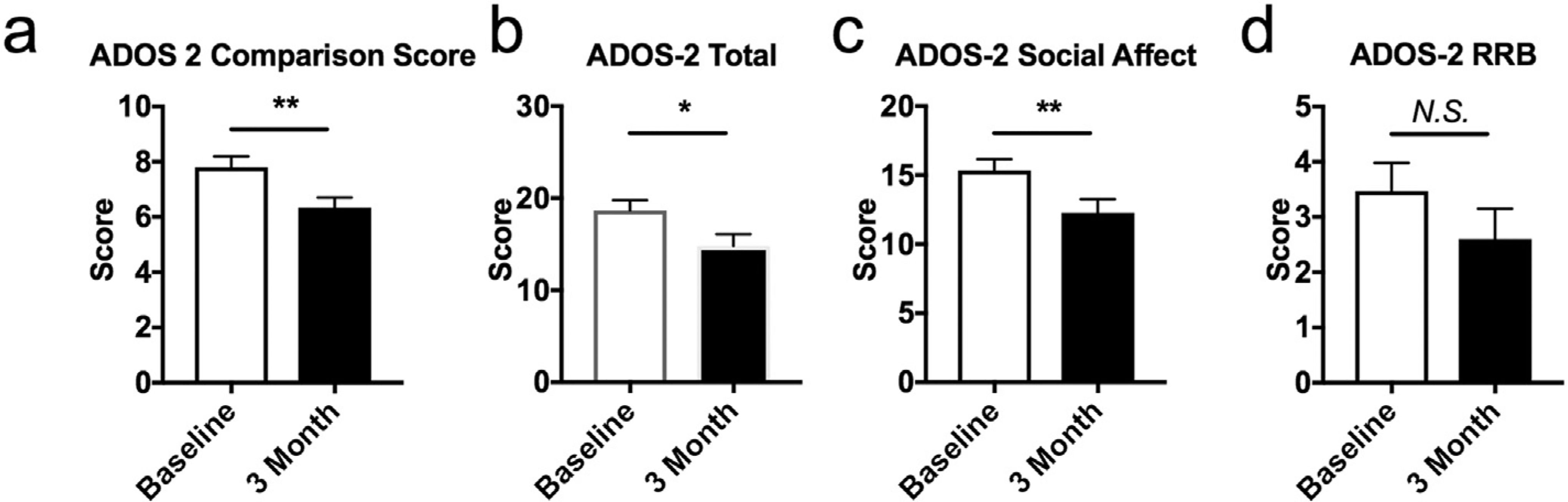
| Autism spectrum |
15 children, 3-month KD |
ADOS-2 significant improvement |
p=0.006 at 3 mo;
sustained at 6 mo |
Lee 2018 |
Note: Published data derive from ketogenic diet interventions. SNV-301 aims to replicate these
metabolic effects via exogenous ketone delivery with improved compliance, titratability, and
exposure control. No clinical trials of SNV-301 have been completed.
3. Published Clinical Data
4. Mechanism: Why Metabolic Correction Resolves Psychiatric Symptoms
The therapeutic effect of ketone bodies in psychiatric illness operates through multiple
convergent mechanisms, each independently validated in human or preclinical systems:
| Mechanism |
Pathway |
Psychiatric Relevance |
| Bioenergetic restoration |
Beta-hydroxybutyrate bypasses impaired glycolysis; direct mitochondrial substrate
via succinyl-CoA:3-ketoacid CoA transferase |
Corrects cerebral glucose hypometabolism documented in schizophrenia, bipolar, MDD |
| NLRP3 inflammasome blockade |
BHB directly inhibits NLRP3 assembly, reducing IL-1beta and IL-18
Youm 2015
|
Neuroinflammation implicated in treatment resistance across diagnoses; CRP
reduced 61% in TRS case |
| Insulin sensitization |
Reduces hepatic glucose output; improves peripheral and central insulin signaling |
HOMA-IR reduced 69% in TRS; insulin resistance 2-3x more prevalent in psychiatric
populations |
| GABA/glutamate modulation |
Acetoacetate inhibits vesicular glutamate transport (VGLUT);
shifts excitatory/inhibitory balance
Juge 2010
|
Glutamate excitotoxicity implicated in psychosis, mood instability, and seizure-
psychiatric comorbidity |
| Epigenetic reprogramming |
BHB acts as endogenous HDAC inhibitor; lysine beta-hydroxybutyrylation modulates
gene expression
Xie 2016
|
Epigenetic dysregulation documented in bipolar disorder, schizophrenia, and MDD |
| BDNF upregulation |
Ketosis increases brain-derived neurotrophic factor via beta-hydroxybutyrylation
of BDNF promoter regions |
BDNF deficiency is among the most replicated findings in depression and
schizophrenia |
| Gut-brain axis |
Shifts microbiome composition; reduces gut permeability and systemic
endotoxemia |
Gut dysbiosis and LPS translocation documented in depression, bipolar, and
alcohol use disorder |
The Convergence
These are not seven separate drug targets. They are seven downstream consequences of a single
upstream intervention: restoring bioenergetic capacity in metabolically compromised neural
tissue. This is why a single metabolic correction produces remissions across diagnostic
categories that share no neurotransmitter target but all share metabolic pathology.
5. Indication Coverage
Published human evidence now spans seven psychiatric categories. The transdiagnostic nature
of the metabolic effect is consistent with the mechanistic hypothesis: if the upstream
pathology is metabolic, the downstream symptom category is secondary.
Documented Human Remissions
Treatment-resistant depression (complete PHQ-9 remission)
Schizoaffective disorder (full remission, deprescription)
Bipolar disorder (PANSS 46% reduction; sustained remission)
OCD (Y-BOCS 0, FOCI 0)
Anorexia nervosa (weight restoration, symptom cessation)
Transdiagnostic (PTSD + ADHD + BED: all scales to 0)
Significant Improvement Documented
Autism spectrum (ADOS-2 improvement, p=0.006)
Alcohol use disorder (craving reduction; metabolic normalization)
Treatment-resistant schizophrenia (metabolic + EPS improvement)
GAD (GAD-7 remission in multiple case series)
PTSD (PCL-5 reduction documented)
ADHD (symptom resolution as part of transdiagnostic response)
6. Clinical Development Plan
Lead Indication: Treatment-Resistant Bipolar Depression
Treatment-resistant bipolar depression was selected as the lead indication based on strength of
existing clinical signal (46% PANSS reduction in controlled inpatient setting), high unmet need
(current options limited to ECT, ketamine, or clozapine), and regulatory precedent for 505(b)(2)
pathways in metabolic therapeutics. Fast Track and Breakthrough Therapy designations may be
available given documented remissions in patients who failed standard of care.
Phase 1a
SAD/MAD safety and PK in healthy volunteers. Establish dose range producing
sustained BHB ≥ 1.5 mM for ≥ 8 hours.
Phase 1b
Open-label in treatment-resistant bipolar depression (n=20-30). Primary: MADRS
change from baseline. Secondary: CGI-S, metabolic biomarkers (HOMA-IR, CRP, ketone AUC).
Phase 2
Randomized, placebo-controlled in TR bipolar depression (n=80-120). 12-week
treatment. Co-primary: MADRS and CGI-S. Biomarker-stratified analysis by baseline
insulin resistance.
Expansion
Schizoaffective disorder (PANSS), alcohol use disorder (heavy drinking days),
and autism spectrum (ADOS-2) as follow-on indications based on Phase 2 signal.
Regulatory Pathway
505(b)(2) leveraging established safety of ketone bodies and extensive dietary intervention
literature. The known safety profile of beta-hydroxybutyrate as an endogenous metabolite
and GRAS-status food ingredient de-risks early clinical development. Orphan Drug
Designation may apply to treatment-resistant subtypes.
The Ask
Development partner for treatment-resistant
psychiatric disorders.
Seeking a CNS-focused pharma partner to co-develop SNV-301 through Phase 2
proof-of-concept in treatment-resistant bipolar depression. Estimated program cost
through Phase 2 readout: ~$20-30M. Structure: co-development partnership with option
to license, or strategic co-lead.
Contact: joel@senoviabiosciences.com
References
1. Danan A, Westman EC, Saslow LR, Ede G. The Ketogenic Diet for Refractory Mental Illness:
A Retrospective Analysis of 31 Inpatients. Front Psychiatry. 2022;13:951376.
PMID: 35873236
2. Laurent N, Bellamy EL, Tague KA, Hristova D, Houston A. Ketogenic metabolic therapy for schizoaffective disorder: a retrospective case series.
Front Nutr. 2025.
PMID: 39990610
3. Needham N, et al. Complete remission of depression and anxiety using a ketogenic diet: case series.
Front Nutr. 2024.
PMID: 38887496
4. Lee RWY, et al. A modified ketogenic gluten-free diet with MCT improves behavior in children
with autism spectrum disorder. Physiol Behav. 2018;188:205-211.
PMID: 29421589
5. Youm YH, et al. The ketone metabolite beta-hydroxybutyrate blocks NLRP3 inflammasome-mediated
inflammatory disease. Nat Med. 2015;21(3):263-269.
PMID: 25686106
6. Juge N, et al. Metabolic control of vesicular glutamate transport and release.
Neuron. 2010;68(1):99-112.
PMID: 20920794
7. Xie Z, et al. Metabolic regulation of gene expression by histone lysine
beta-hydroxybutyrylation. Mol Cell. 2016;62(2):194-206.
PMID: 27105115
8. Laurent N, Bellamy EL, Hristova D, Houston A. Ketogenic metabolic therapy in the remission of chronic major depressive disorder:
a retrospective case study. Front Nutr. 2025.
PMID: 40083888
9. Transdiagnostic remission of comorbid PTSD, ADHD, and binge-eating disorder
following ketogenic metabolic therapy. 2025.
PMID: 40626225
10. OCD and ulcerative colitis remission with ketogenic diet. 2025.
PMID: 40248603
11. Metabolic normalization in treatment-resistant schizophrenia. 2025.
PMID: 41356674
12. Evangeliou A, et al. Application of a ketogenic diet in children with autistic behavior.
J Child Neurol. 2003;18(2):113-118.
PMID: 12693778
Senovia Biosciences ·
joel@senoviabiosciences.com
SNV-301 is investigational. No clinical trials of SNV-301 have been completed.
Published evidence derives from ketogenic diet interventions.
Last updated: February 2026 | Version 4.0