Therapeutic Ketosis for Drug-Resistant Epilepsy
Translating 100 Years of Ketogenic Medicine into a Titratable Pharmaceutical
Clinical Evidence Platform | February 2026
Contents
- 1. The Opportunity: A Proven Mechanism Without a Drug
- 2. Human Clinical Validation (RCTs + Meta-Analysis)
- 3. Literature Corpus: Comprehensive Analysis
- 4. The Mechanism: Why Ketones Stop Seizures
- 5. The Drug Development Gap
- 6. Human PK Advantage: Extended Duration
- 7. Target Indications: The DEE Basket
- 8. Regulatory Pathway: 505(b)(2)
- 9. Clinical Development Framework
- References
The Opportunity
The ketogenic diet has been used to treat epilepsy since the 1920s.
Cochrane meta-analysis confirms
RR 5.80 for seizure reduction (4 RCTs; 385 patients; p<0.001). Yet no pharmaceutical exists to
replicate this effect. Modern ketone prodrug chemistry can now deliver sustained therapeutic
ketosis in a titratable, drug-like format—potentially unlocking a multi-billion dollar
opportunity in drug-resistant epilepsy.
RR 5.8
Cochrane Risk Ratio
(4 RCTs)
38%
Responder Rate
(Neal 2008 RCT)
100+
Years of Clinical
Validation
~85,000
US DEE Patients
Addressable
1. The Opportunity: A Proven Mechanism Without a Drug
Drug-resistant epilepsy affects approximately 30% of epilepsy patients. After 2+ failed antiseizure medications,
the probability of achieving seizure freedom with additional drugs drops dramatically. The ketogenic diet
offers a fundamentally different mechanism—metabolic state change rather than single receptor
targeting—with responder rates that rival or exceed late-stage ASMs.
The Longboard Pharma Parallel: Longboard Pharmaceuticals achieved a $2.6 billion
acquisition by Lundbeck based on Phase 2 DEE basket trial data. The ketogenic diet has
superior historical responder rates (38-54% across syndromes) to most novel ASM mechanisms,
yet no pharmaceutical currently exploits this biology.
The Problem: Diet Is Not Scalable
- Requires 90% fat, <20g carbs/day
- Median adherence: <12 months
- Requires specialized dietitian support
- Social isolation, quality of life impact
- Only ~15,000 US patients on KD today
The Solution: Pharmaceutical Ketosis
- Oral drinkable prodrug (BID dosing)
- No dietary restriction required
- Titratable to blood ketone target
- Measurable PD endpoint (fingerstick ketones)
- Scalable to 85,000+ US DEE patients
2. Human Clinical Validation: Gold-Standard RCT Evidence
| Study |
Design |
Population |
Responder Rate |
P-Value |
Neal 2008
PMID: 18456557 |
RCT (n=145)
3 months |
Drug-resistant pediatric |
38% vs. 6% |
p<0.0001 |
Martin-McGill 2020
PMID: 32588435 |
Cochrane Meta-Analysis
4 RCTs (n=385) |
Drug-resistant pediatric |
RR 5.80
(95% CI 3.48–9.65) |
P < 0.001 |
Lambrechts 2017
PMID: 27027847 |
RCT (n=48) |
Refractory childhood |
KD superiority confirmed |
Significant |
Qiao 2025
PMC11960278 |
Retrospective (n=213) |
Pediatric KD |
Optimal range defined |
BHB 1.1–4.9 mM |
Context: A Risk Ratio of 5.80 means patients on ketogenic therapy were nearly 6× more
likely to achieve ≥50% seizure reduction than controls. This effect size is among the largest
documented for any epilepsy intervention in drug-resistant populations.
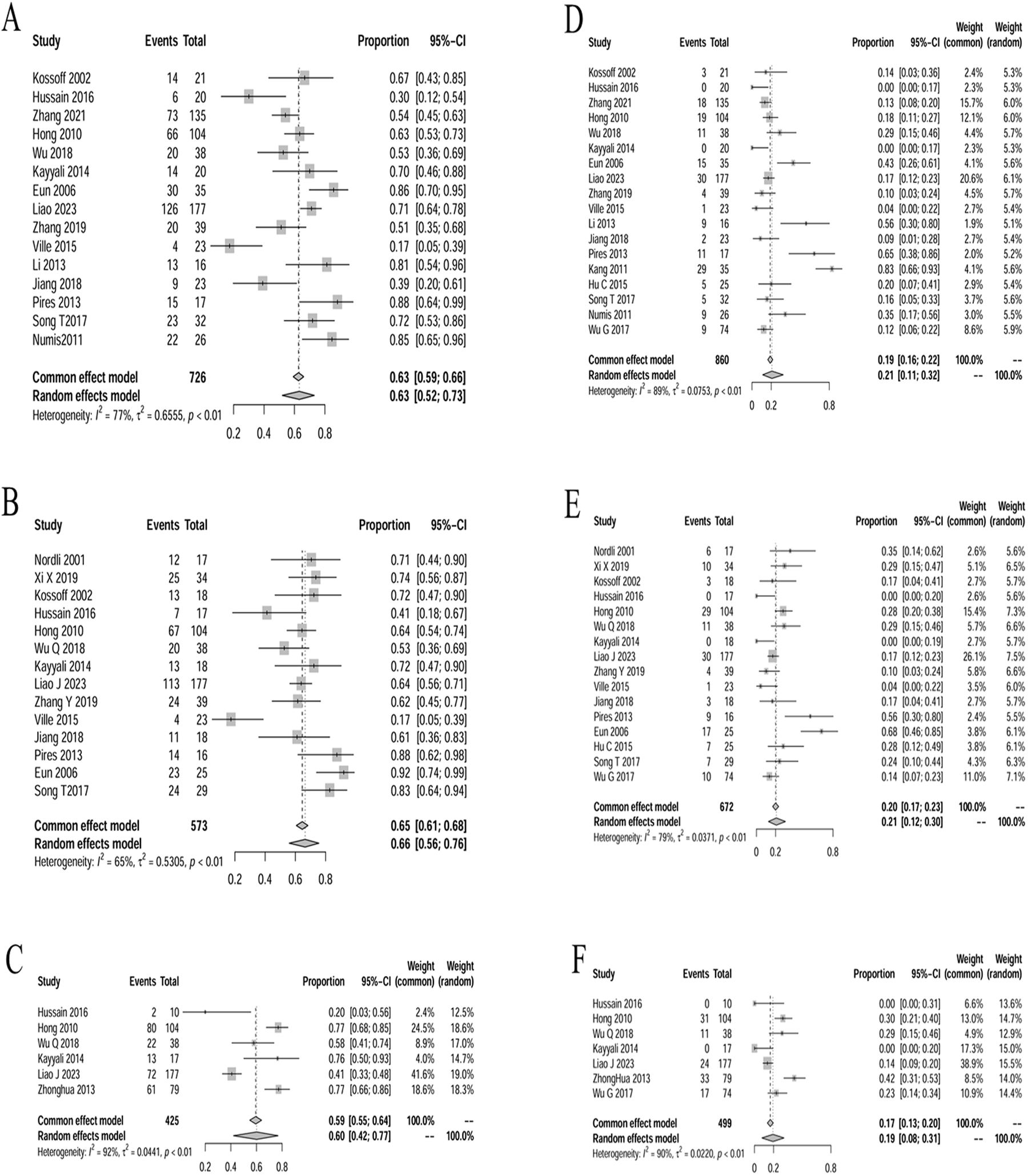
Published Efficacy Data: Meta-Analysis of Seizure Outcomes
Zuo et al. (2025) conducted a comprehensive meta-analysis of ketogenic diet therapy in infantile epileptic spasm syndrome, pooling data from 726 patients across 15+ studies. The forest plots below show seizure reduction rates at multiple follow-up timepoints.
3. Literature Corpus: Comprehensive Systematic Analysis
1,370
Full-texts Acquired
| Outcome |
Finding |
Clinical Significance |
| Seizure Reduction |
~50% mean reduction in refractory cohorts |
Primary efficacy endpoint |
| Seizure Freedom |
10–32% in DEEs; up to 54% in Doose syndrome |
Disease modification signal |
| Cognitive/Behavioral |
Improved alertness, verbal function, sleep |
Quality of life benefit |
| Survival/SUDEP |
Extended survival in Dravet models; SUDEP reduction |
Mortality benefit |
4. The Mechanism: Why Ketones Stop Seizures
Ketogenic therapy works through 8+ distinct mechanistic pathways—a fundamentally
different approach from single-target ASMs. This multi-pathway profile may explain efficacy in
drug-resistant populations where single-target agents fail.
| Target |
Threshold |
Mechanism |
Citation |
| VGLUT1/2 |
IC₅₀ ~0.2 mM |
Reduces glutamate loading → decreased excitatory transmission |
Juge 2010 (PMID: 20920794) |
| NLRP3 Inflammasome |
≥1.0 mM |
Inhibits inflammasome → reduces IL-1β neuroinflammation |
Youm 2015 (PMID: 25686106) |
| K-ATP Channels |
~2.0 mM |
Hyperpolarizes neurons → raises seizure threshold |
Ma 2007 (PMID: 17409226) |
| HCAR2/GPR109A |
EC₅₀ ~0.7 mM |
Neuroprotective GPCR signaling |
Taggart 2005 (PMID: 15929991) |
| HDAC Class I |
IC₅₀ 2–5 mM |
Epigenetic modulation |
Shimazu 2013 (PMID: 23223453) |
| Gut-Brain Axis |
Variable |
GABA modulation via microbiota |
Olson 2018 (PMID: 29804833) |
Key Insight: Juge 2010 demonstrated that acetoacetate inhibits vesicular glutamate transporters
with an IC₅₀ of ~0.2 mM—a concentration readily achievable with oral ketone prodrugs. This directly reduces
excitatory neurotransmission at the presynaptic level.
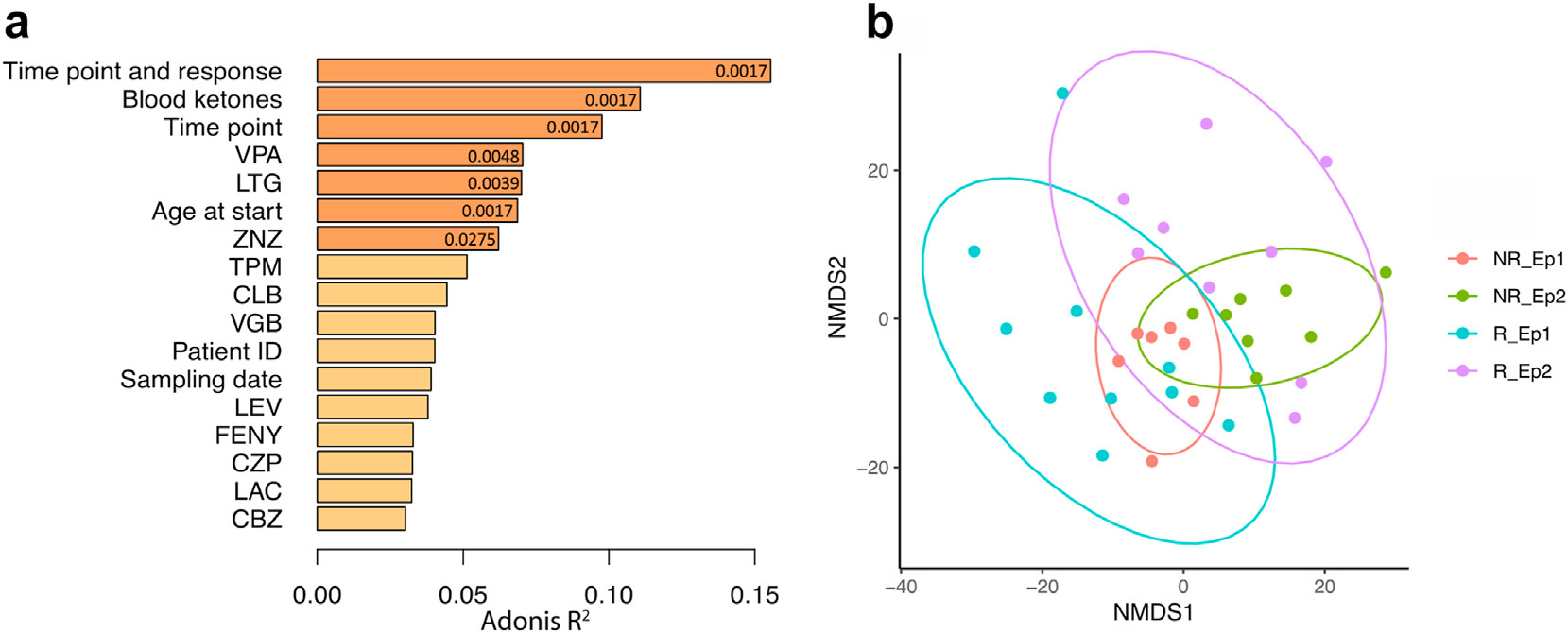
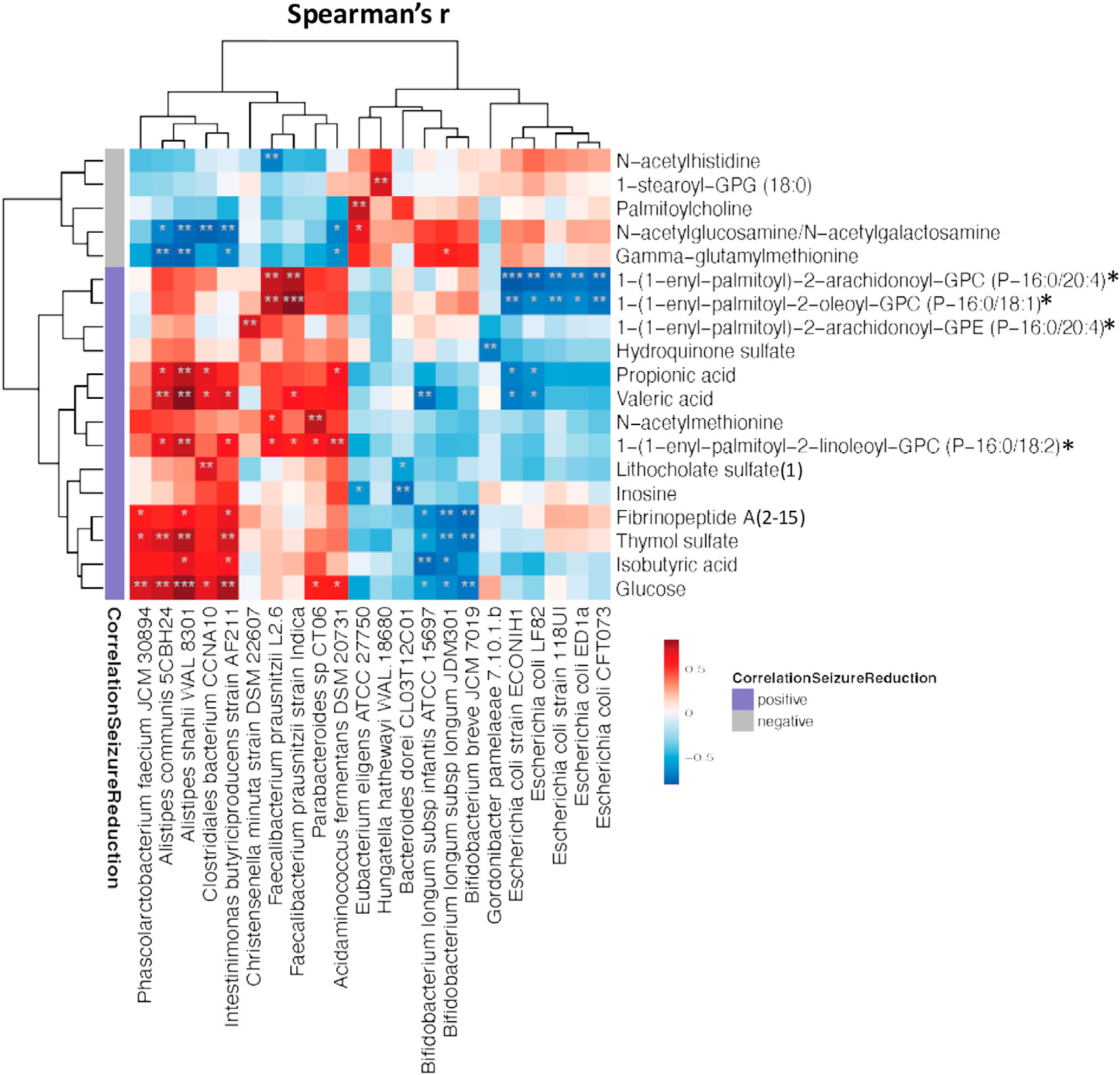
Multi-Mechanism Convergence: Metabolomics Evidence
The ketogenic diet's anticonvulsant efficacy is not attributable to any single pathway. Therapeutic ketosis simultaneously engages at least six distinct mechanisms, each operating at different BHB concentrations. SNV-401 achieves exposure levels that activate all of them.
The primary anticonvulsant mechanism is VGLUT inhibition (Juge 2010): acetoacetate directly blocks vesicular glutamate transporters at IC₅₀ ~0.2 mM, reducing glutamate loading into synaptic vesicles. This concentration is achievable with a single oral dose. Neuroinflammatory suppression via NLRP3 blockade (Youm 2015, PMID: 25686106) operates in parallel at higher BHB concentrations (~1.0 mM), reducing IL-1β-driven seizure susceptibility.
5. The Drug Development Gap: Why Prior Products Failed
| Prior Approach |
Peak Ketones |
Duration |
Why It Failed |
| Ketone Salts |
0.5–1.0 mM |
<2h |
Sub-therapeutic exposure; 4–8g Na⁺/day limits dosing |
| MCT Oil |
~0.5 mM |
<1h |
Sub-therapeutic; GI tolerability limits escalation |
| 1,3-Butanediol Esters |
2–3 mM |
2–4h |
Metabolic concerns limit chronic use; short duration |
| Novel Ketone Prodrugs |
1.8–2.5 mM |
8–14h |
Extended half-life in humans enables BID dosing |
The Human Advantage: Ketone half-life is 20–35× longer in humans than rodents (Clarke 2012,
PMID: 22561291). This pharmacokinetic reality enables practical BID dosing with ~95% daily therapeutic coverage.
6. Human PK Advantage: Extended Duration Profile
| Dosing Scenario |
Daily Dose |
Peak Ketones |
Duration >0.5 mM |
Daily Coverage |
| QD Fasted |
28g |
1.8–2.5 mM |
10–14h |
~50% |
| ★ BID (AM Fasted + PM Fed) |
56g/day |
1.5–2.5 mM |
~20h total |
~95% |
7. Target Indications: The DEE Basket
| Indication |
US Patients |
KD Response Rate |
ODD |
| GLUT1 Deficiency |
~4,000 |
Standard of Care—majority seizure-free (Klepper 2005) |
✓ |
| Dravet Syndrome |
~16,000 |
32.5% seizure-free at 3 months |
✓ |
| Lennox-Gastaut |
~48,000 |
40% responders; 15% seizure-free at 18 mo |
✓ |
| Doose Syndrome |
~5,000 |
54% seizure-free; 86% >70% reduction |
✓ |
| Angelman Syndrome |
~15,000 |
5/6 patients >80% reduction (Thibert 2012) |
✓ |
| Mitochondrial Epilepsy |
~2,000 |
74% responders overall; 93% in mtDNA subgroup |
✓ |
Total Addressable Market: ~85,000 US patients across DEE indications. With orphan pricing
($200K+/year) and 7-year exclusivity per indication, the commercial opportunity is multi-billion
dollars.
8. Regulatory Pathway: 505(b)(2) with Strong Precedent
505(b)(2) Rationale
- Precedent: Dojolvi (triheptanoin) approved 2020
- Rationale: Endogenous metabolite + literature
- Strategy: Reference 100+ years of KD data
Orphan Incentives (per indication)
- 7 years market exclusivity
- Tax credits for clinical costs
- Waived PDUFA fees ($3M+ value)
- Orphan pricing power ($200K+/yr)
9. Clinical Development Framework
| Phase |
Design |
Key Endpoints |
| Phase 1a |
SAD/MAD in healthy volunteers (n=24-48) |
PK confirmation; dose proportionality |
| Phase 1b |
DRE patients (n=12-24) |
Seizure frequency + PK/PD correlation |
| Phase 2 |
DEE basket (Dravet, LGS, GLUT1-DS, Angelman) |
Median % change seizure frequency |
Go/No-Go Criteria (Phase 1)
| Parameter |
GO Threshold |
Rationale |
| Peak ketones (fasted) |
≥1.5 mM |
Therapeutic exposure achieved |
| Duration >0.5 mM |
≥8 hours/dose |
Human t½ advantage confirmed |
| GI tolerability |
<20% Grade 2+ AEs |
Chronic use feasibility |
Summary: The Evidence Speaks
- Cochrane-level validation: RR 5.80 across 4 RCTs—one of the largest effect sizes in DRE
- 100+ years of clinical experience: Mechanism proven, just never pharmaceuticalized
- Multi-pathway mechanism: Addresses why single-target ASMs fail in refractory patients
- Clear PK opportunity: Human half-life enables practical BID dosing
- Multi-billion dollar franchise: ~85,000 US patients across orphan DEE indications
This is validated biology awaiting modern drug development.
Appendix: Complete References
Landmark Clinical Trials
- Neal EG et al. (2008). The ketogenic diet for treatment of childhood epilepsy: RCT. Lancet Neurol.
PMID: 18456557
- Martin-McGill KJ et al. (2020). Ketogenic diets for drug-resistant epilepsy. Cochrane Database Syst
Rev. PMID: 32588435
- Lambrechts DA et al. (2017). RCT of ketogenic diet in refractory childhood epilepsy. Epilepsia
Open. PMID: 27027847
- Gilbert DL et al. (2000). Blood β-hydroxybutyrate and seizure control. J Child Neurol.
PMID: 11198492
- Qiao X et al. (2025). Therapeutic range for pediatric KD. PMC11960278
Mechanism: Acetoacetate/VGLUT Inhibition
- Rho JM et al. (2002). AcAc anticonvulsant action in vivo. Epilepsia. PMID:
11952765
- Juge N et al. (2010). VGLUT inhibition by acetoacetate. Neuron. PMID: 20920794
- D'Agostino DP et al. (2013). Ketone esters increase seizure latency. Neuroscience. PMID:
23552496
- Veech RL et al. (2017). Ketone metabolism and NAD+. IUBMB Life. PMID: 28371201
Multi-Pathway Mechanisms
- Youm YH et al. (2015). BHB blocks NLRP3 inflammasome. Nat Med. PMID: 25686106
- Shimazu T et al. (2013). BHB as HDAC inhibitor. Science. PMID: 23223453
- Ma W et al. (2007). K-ATP channels in KD. PMID: 17409226
- Olson CA et al. (2018). Gut microbiome mediates KD anti-seizure effect. Cell. PMID:
29804833
- Bough KJ et al. (2006). Mitochondrial biogenesis. J Neurosci. PMID: 16807920
- Taggart AK et al. (2005). HCAR2/GPR109A activation by BHB. PMID: 15929991
PK & Safety
- Clarke K et al. (2012). Kinetics, safety and tolerability of (R)-3-hydroxybutyl (R)-3-hydroxybutyrate in
healthy adult subjects. Regul Toxicol Pharmacol. PMID: 22561291
- Stubbs BJ et al. (2017). On the metabolism of exogenous ketones in humans. Front Physiol.
PMID: 29163194
- Soto-Mota A et al. (2019). Safety and tolerability of sustained exogenous ketosis using ketone monoester.
Regul Toxicol Pharmacol. PMID: 31655093
Indication-Specific Evidence
- Klepper J (2005). GLUT1 deficiency syndrome. Neuropediatrics. PMID: 16217704
- Dravet study (2023). KD in Dravet syndrome: 32.5% seizure-free at 3 mo. PMID: 37060636
- Caraballo RH et al. (2014). KD in Lennox-Gastaut syndrome: 40% responder, 15% seizure-free at 18 mo.
PMID: 25011392
- Stenger E et al. (2017). KD in Doose syndrome/MAE: 54% seizure-free, 86% responders. PMID:
28273610
- Thibert RL et al. (2012). Low glycemic index treatment in Angelman syndrome. PMID: 22779920
- Huang et al. (2022). Efficacy of ketogenic diet for mitochondrial epilepsy. Front Neurol.
PMID: 35979062
Published Meta-Analyses & Metabolomics
- Zuo CX et al. (2025). The efficacy and safety of the ketogenic diet in infantile epileptic spasm syndrome: a meta-analysis. European Journal of Epilepsy. DOI: 10.1016/j.seizure.2025.01.022
- Carroll JH et al. (2025). Over twenty-five years of ketogenic diet therapy: Supporting children and adults with drug-resistant epilepsy. Epilepsy & Behavior. DOI: 10.1016/j.yebeh.2025.110268
- Dahlin M, Wheelock CE, Prast-Nielsen S (2024). Association between seizure reduction during ketogenic diet treatment and changes in circulatory metabolites and gut microbiota. EBioMedicine (Lancet). DOI: 10.1016/j.ebiom.2024.105436
Regulatory & Market
- FDA Dojolvi Approval (NDA 213687). FDA Access Data [citing 505(b)(2) pathway].
- Lundbeck acquires Longboard Pharmaceuticals for $2.6B. Lundbeck Newsroom 2024.
Clinical Evidence Platform | February 2026
Key Citations: Neal 2008, Martin-McGill 2020 (Cochrane), Juge 2010, Clarke 2012, D'Agostino 2013
The Ask
Orphan indication partner for DEE basket (Dravet, LGS, GLUT1-DS)
Longboard Pharmaceuticals $2.6B exit validates the metabolic epilepsy path
joel@senoviabiosciences.com