SNV-801: The Metabolic Inotrope — Restoring Cardiac Energetics via Oral Acetoacetate Delivery
A First-in-Class Approach to Myocardial Bioenergetic Rescue
Senovia Biosciences, Inc. | Scientific Brief
+2.0 L/min
Cardiac Output
Nielsen 2019
+8 pts
LVEF (absolute)
Nielsen 2019
−5 mmHg
Peak PCWP
Gopalasingam 2024
~50%
Infarct Reduction
Chu 2024
Executive Summary
The failing heart suffers from a fundamental deficit of ATP production. Multiple randomized controlled trials
now demonstrate that exogenous ketones produce reproducible, dose-dependent hemodynamic improvements across
the heart failure spectrum—from stable chronic disease to cardiogenic shock. These effects rival the
magnitude of inotropic support, without the associated arrhythmogenic risk.
SNV-801 is an oral acetoacetate-releasing prodrug designed to achieve sustained therapeutic
ketosis (1.0–3.5 mM). Unlike β-hydroxybutyrate (BHB), acetoacetate enters cardiac oxidation without
consuming NAD⁺ and in fact regenerates NAD⁺, restoring the redox balance that the failing
heart critically requires. This brief summarizes the human clinical evidence and mechanistic rationale
supporting this approach.
Clinical Evidence
Human evidence: 6 completed randomized controlled trials in human heart failure
Status: Seeking strategic partner for registration-quality Phase 2b trial
The Therapeutic Rationale
Heart failure is increasingly understood as a disease of metabolic inflexibility. The healthy heart is
omnivorous, deriving ATP from fatty acids, glucose, lactate, and ketones depending on availability. In the
failing heart, this flexibility is lost—substrate utilization becomes constrained, ATP production falls, and
contractile function declines accordingly.1
SGLT2 inhibitors, now standard of care across the heart failure spectrum, mildly elevate circulating ketones
(0.1–0.3 mM). Mechanistic studies suggest this metabolic shift contributes meaningfully to their cardiovascular
benefit, independent of their glucosuric and natriuretic effects.2 This observation raises an
important question: what would happen if we delivered therapeutic-level ketones directly?
The clinical evidence now provides a clear answer.
Human Clinical Evidence
Six randomized, controlled studies have evaluated exogenous ketone administration in patients with heart failure.
Across populations ranging from stable outpatients to ICU-admitted cardiogenic shock, the hemodynamic response
is consistent: improved cardiac output, improved filling pressures, and reduced biomarkers of myocardial stress.
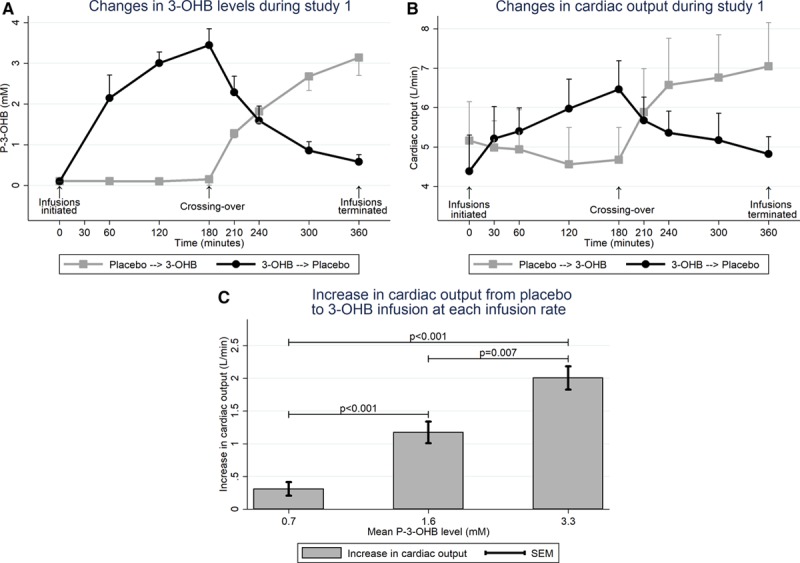
Study 1: Acute Intravenous 3-OHB in Chronic HFrEF
Nielsen et al., Circulation 2019
Randomized crossover, n=16 | PMID: 30884964
Patients with chronic HFrEF (EF 32±7%) received 3-hour intravenous 3-hydroxybutyrate infusion versus
isocaloric glucose control, on background guideline-directed medical therapy. Peak circulating BHB reached
approximately 3.3 mM.
+2.0 L/min
Cardiac Output
−18%
Systemic Vascular Resistance
Myocardial external efficiency remained unchanged, indicating
that the improved hemodynamics occurred without an increase in oxygen consumption.
Study 2: Ketone Ester in Cardiogenic Shock
Berg-Hansen et al., JACC Heart Failure 2023
Double-blind crossover, n=12 | PMID: 37452805
ICU patients with cardiogenic shock received a single enteral ketone ester bolus versus maltodextrin placebo,
with invasive pulmonary artery catheter monitoring. All patients were on mechanical or pharmacological
circulatory support.
+4 pts
LVEF (95% CI: 2–6)
+0.07 W
Cardiac Power Output
This represents acute biventricular improvement in the
highest-acuity population studied—patients already receiving maximal conventional support.
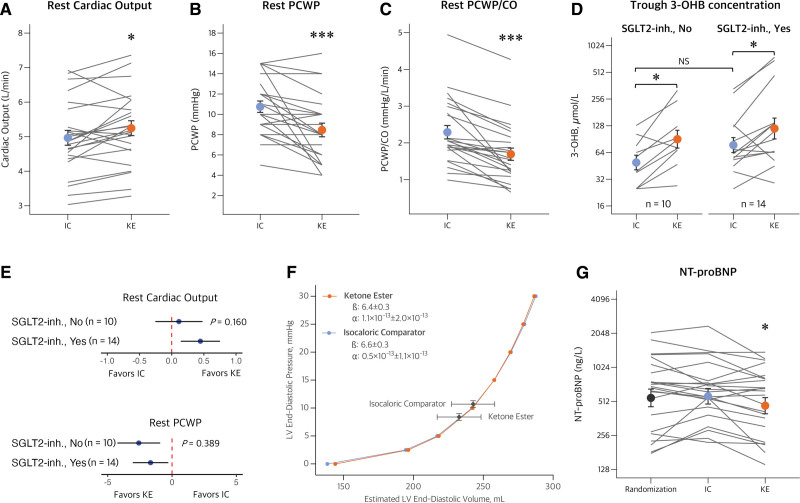
Study 3: 14-Day Oral Ketone Ester in Stable HFrEF
Berg-Hansen et al., Circulation 2024
Randomized double-blind crossover, n=24 | PMID: 38533643
Patients with stable HFrEF on optimal guideline-directed therapy received oral ketone ester (4 doses daily ×
14 days) versus isocaloric comparator, with invasive hemodynamic assessment at baseline and follow-up.
+0.3 L/min
Resting CO (trough)
+3 pts
LVEF (exploratory)
Study 4: 2-Week Oral Ketone Ester in HFpEF with Type 2 Diabetes
Gopalasingam et al., Circulation 2024
Randomized double-blind crossover, n=24 | PMID: 39162035
Patients with HFpEF and comorbid type 2 diabetes received oral ketone ester versus placebo for 14 days, with
invasive exercise hemodynamic testing.
−5 mmHg
Peak Exercise PCWP
+10 mL
Peak Stroke Volume
The reduction in peak exercise PCWP and the right-shift of the
end-diastolic pressure-volume relationship suggest both improved hemodynamics and reduced diastolic
stiffness—a particularly meaningful finding in HFpEF.
Study 5: Oral 1,3-Butanediol in HFrEF
Guldbrandsen et al., JAHA 2025
Randomized crossover, n=12 | PMID: 39719429
Single oral dose of (R)-1,3-butanediol (0.5 g/kg) versus placebo, with 6-hour echocardiographic monitoring.
+0.9 L/min
Cardiac Output (95% CI: 0.7–1.1)
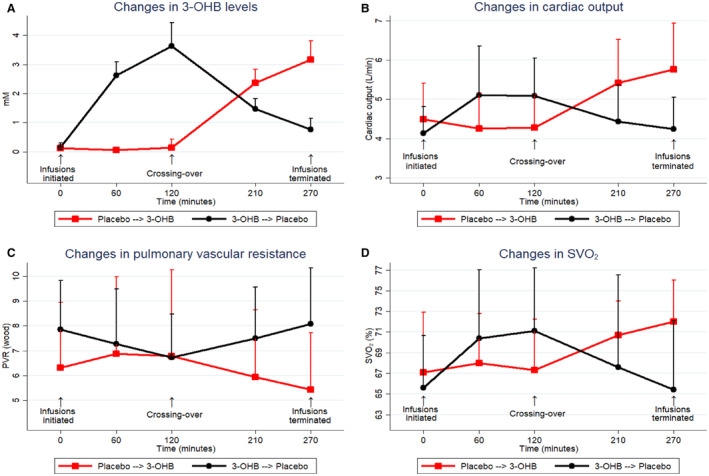
Study 6: Pulmonary Hypertension
Nielsen et al., JAHA 2023
Randomized crossover, n=10 | PMID: 37183871
Patients with pulmonary arterial hypertension or chronic thromboembolic pulmonary hypertension received
2-hour IV 3-OHB infusion versus saline, with invasive right heart catheterization.
+1.2 L/min
Cardiac Output (+27%)
Simultaneous improvement in cardiac output and reduction in
pulmonary vascular resistance—a desirable "inodilator" profile—was observed acutely.
Target Engagement: Multi-Mechanistic Profile
SNV-801 engages multiple validated molecular targets relevant to cardiac pathophysiology. The table below
summarizes the key mechanisms and their relevance to heart failure.
Cardiac Target Engagement Matrix
| Molecular Target |
Primary Ligand |
Threshold |
Cardiac Effect |
Biomarker/Endpoint |
| ATP Synthesis |
Total Ketones |
≥0.5 mM |
Restores myocardial ATP in energy-starved failure |
Ejection Fraction, CO |
| NAD⁺ Regeneration |
Acetoacetate |
Ratio-dependent |
Generates NAD⁺; restores mitochondrial redox |
Efficiency metrics |
| NLRP3 Inflammasome |
BHB |
≥1.0 mM |
Inhibits sterile inflammation post-infarct |
hs-CRP, IL-1β |
| HDAC Inhibition |
BHB |
~1.0–2.0 mM |
Reduces cardiac fibrosis and adverse remodeling |
Cardiac MRI (fibrosis) |
| SIRT3 Activation |
BHB |
≥0.5 mM |
Restores mitochondrial protein acetylation balance |
Oxidative stress markers |
| HCA2/GPR109A |
BHB |
EC₅₀ ~0.7 mM |
Cardioprotective GPCR signaling (vasodilation) |
SVR, Blood Pressure |
| mTOR Inhibition |
BHB |
≥1.0 mM |
Activates autophagy; reduces infarct size at reperfusion |
Infarct size |
SNV-801 is designed to achieve sustained 1.0–3.5 mM
ketosis, engaging all listed targets at therapeutic exposures.
Mechanistic Rationale for Acetoacetate
The clinical evidence for ketone-based hemodynamic improvement is now substantial. The question is how to
translate this into an optimized therapeutic.
Circulating ketones exist as two interconvertible species: β-hydroxybutyrate (BHB) and acetoacetate (AcAc).
In the heart, BHB is oxidized to acetoacetate by the mitochondrial enzyme β-hydroxybutyrate dehydrogenase
(BDH1). This reaction consumes NAD⁺, converting it to NADH.
In the heart failure state, the NAD⁺/NADH ratio is already depressed—a contributing factor to impaired
mitochondrial function. Delivering BHB as the exogenous ketone further draws down the NAD⁺ pool at the very
moment of oxidation.
The Acetoacetate Advantage: NAD⁺ Regeneration
Acetoacetate enters myocardial ketolysis downstream of the NAD⁺-consuming step. When the heart
oxidizes AcAc directly, it bypasses BDH1 entirely. More importantly, the oxidation of acetoacetate via
succinyl-CoA:3-ketoacid-CoA transferase (SCOT) and subsequent acetyl-CoA production regenerates
NAD⁺ during mitochondrial electron transport.
This is not merely "NAD⁺ sparing"—acetoacetate delivery actively restores the NAD⁺/NADH
ratio. This is critical for the failing heart, where NAD⁺ depletion impairs sirtuin signaling,
mitochondrial biogenesis, and oxidative phosphorylation efficiency.
Recent work by Koay et al. (Circulation Research 2025) demonstrated that the human heart possesses
intrinsic ketogenic capacity via HMGCS2, and that NAD⁺ repletion therapy in HFpEF models
requires this ketogenic pathway to exert its beneficial effects.3
SNV-801 is designed to deliver acetoacetate directly—providing the myocardium with
NAD⁺-regenerating fuel rather than NAD⁺-consuming BHB.
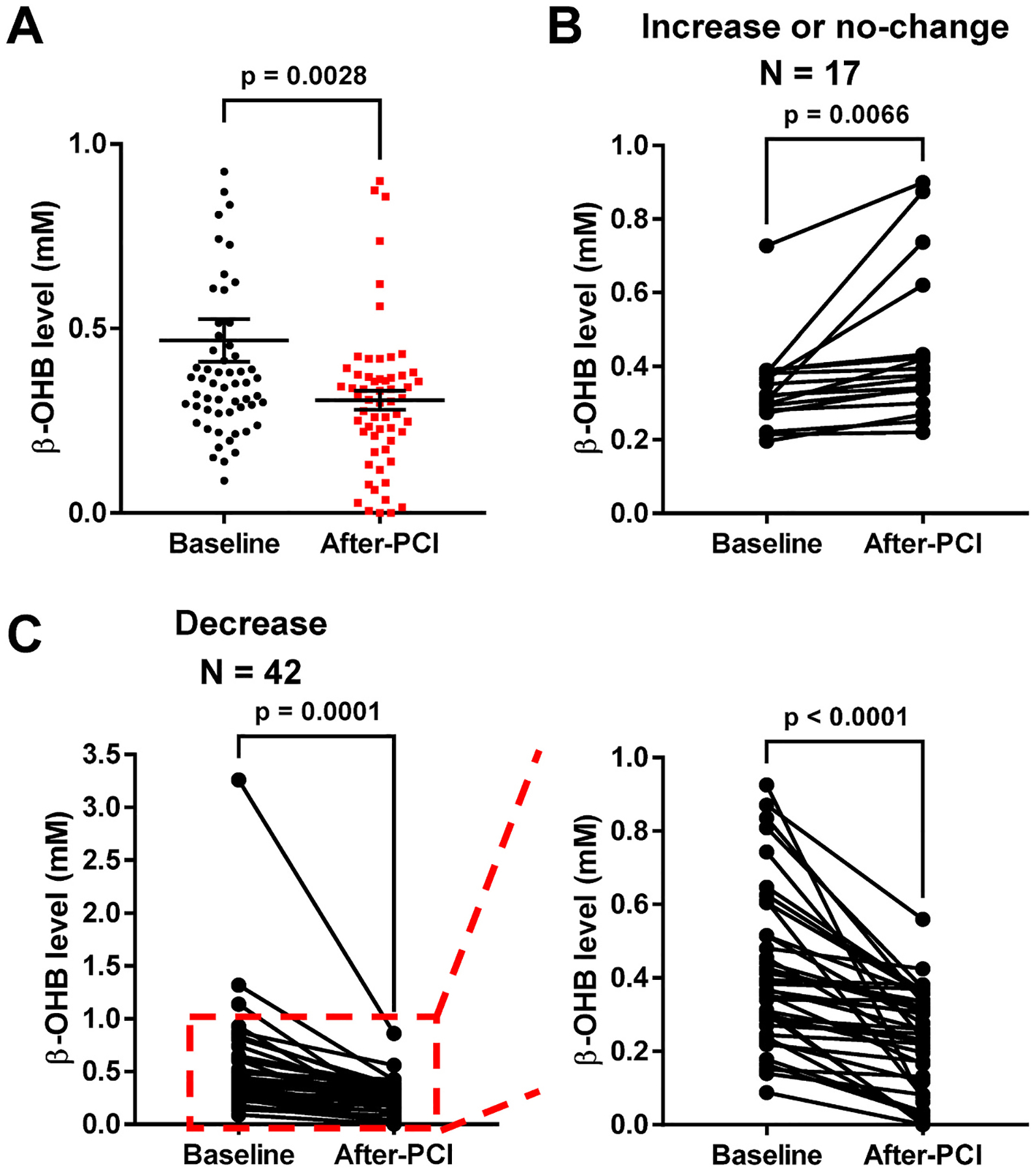
Preclinical Cardioprotection
Complementary preclinical studies provide mechanistic context for the clinical observations and demonstrate
additional therapeutic potential in acute ischemia:
Infarct Size Reduction at Reperfusion
Chu et al., J Mol Cell Cardiol 2024
Mouse I/R Model | PMID: 37979443
β-hydroxybutyrate administered at the moment of reperfusion—modeling clinical scenarios such as post-PCI
treatment—reduced myocardial infarct size by approximately 50%. The mechanism was traced to mTOR
inhibition and activation of cardioprotective autophagy.
Post-MI Reverse Remodeling
Yurista et al., Circ Heart Fail 2021
Rat Post-MI HF Model | PMC: 7819534
In a rat model of post-myocardial infarction heart failure, ketone ester dietary treatment—initiated
after established HF—restored cardiac function dramatically.
Normalized
Myocardial ATP
↓ Fibrosis
Reverse Remodeling
SGLT2i Mechanism: Ketones as the Effector
Ho et al., Circulation 2025
Preclinical + Metabolomics | PMID: 40069113
This study demonstrated that enhanced myocardial ketone body oxidation specifically contributes to the
cardioprotective effects of empagliflozin. When ketone metabolism was blocked, the SGLT2i benefit was
attenuated—providing causal evidence for the "ketone hypothesis" of SGLT2i cardioprotection.
Summary of Clinical Evidence
| Study |
Population |
Design |
n |
BHB |
ΔCO |
ΔLVEF |
ΔPCWP |
Other |
| Nielsen 2019 |
HFrEF |
RCT X-over |
16 |
3.3 mM |
+2.0 L/min |
+8 pts |
— |
SVR −18% |
| Berg-Hansen 2023 |
Shock |
DB X-over |
12 |
KE bolus |
— |
+4 pts |
↓ bivent |
CPO +0.07 W |
| Nielsen 2023 |
PAH |
RCT X-over |
10 |
~3 mM |
+1.2 L/min |
— |
— |
PVR −18% |
| Berg-Hansen 2024 |
HFrEF |
RCT DB 14d |
24 |
1.5–2.5 |
+0.3 L/min |
+3 pts |
−3 mmHg |
BNP −18% |
| Gopalasingam 2024 |
HFpEF+T2D |
RCT DB 14d |
24 |
~1.0 mM |
+0.2 L/min |
— |
−5 peak |
↓LV stiff |
| Guldbrandsen 2025 |
HFrEF |
RCT X-over |
12 |
BD oral |
+0.9 L/min |
+3 pts |
— |
SV +15 mL |
All studies compared exogenous ketone intervention vs. placebo/comparator, on background
standard-of-care therapy. X-over = crossover; DB = double-blind.
SNV-801: Product Profile
| Attribute |
Profile |
| Mechanism |
Oral acetoacetate-releasing prodrug |
| Target Exposure |
1.0–3.5 mM sustained ketosis (therapeutic range) |
| Differentiation |
NAD⁺-regenerating (AcAc bypasses BDH1 and restores NAD⁺/NADH ratio) |
| Lead Indication |
HFpEF (high unmet need); HFrEF (expansion) |
| Expected Endpoints |
Hemodynamic (CO, PCWP); symptom (KCCQ); biomarker (NT-proBNP) |
| Regulatory Path |
505(b)(2) NDA |
Safety Considerations
The target exposure range (1.0–3.5 mM) represents physiological nutritional ketosis, a metabolic state
extensively studied in fasting, ketogenic diet, and supplement contexts. This is distinct from diabetic
ketoacidosis (DKA), which requires the triad of ketones typically >10 mM, metabolic acidosis, and
hyperglycemia—conditions that do not apply to therapeutic ketone administration in euglycemic patients.
Across the six clinical studies summarized above, encompassing nearly 100 patients with heart failure across
a range of acuities, no serious treatment-related adverse events have been reported.
Strategic Positioning
SGLT2 inhibitors have established that mild ketone elevation (0.1–0.3 mM) contributes to cardiovascular
benefit. SNV-801 is designed to deliver approximately 10-fold higher ketone exposure, targeting the
therapeutic range (1.0–3.5 mM) demonstrated to produce clinically meaningful hemodynamic effects in the
randomized trials reviewed above.
This positions SNV-801 as complementary to SGLT2 inhibitor therapy—not competitive with it. SGLT2 inhibitors
address volume and neurohormonal pathways; SNV-801 directly addresses the bioenergetic deficit.
SGLT2i Market Context: The SGLT2i cardiovascular market exceeds $15B annually. Emerging evidence links SGLT2i benefit partly to ketone body elevation (Verma 2019, PMID: 31033127; Ahmed 2023, PMID: 37042253). SNV-801 delivers 10-20x higher ketone exposure than SGLT2i-mediated ketogenesis, positioning it as a synergistic add-on therapy.
Partner Opportunity: Senovia is seeking co-development partners, option-to-license
agreements, or acquisition for SNV-801. A comprehensive data room is available under CDA.
References
- Nielsen R, et al. Cardiovascular Effects of Treatment With the Ketone Body 3-Hydroxybutyrate in
Chronic Heart Failure Patients. Circulation. 2019;139(18):2129-2141. PMID: 30884964
- Ferrannini E, et al. Shift to Fatty Substrates in the Failing Heart. J Am Coll Cardiol.
2016;67(22):2690-2703. PMID: 27018132
- Koay YC, et al. The Heart Has Intrinsic Ketogenic Capacity that Mediates NAD+ Therapy in HFpEF.
Circ Res. 2025;136:1113-1130. PMID: 40211954
- Yurista SR, et al. Ketone Ester Treatment Improves Cardiac Function and Reduces Pathological
Remodeling in Preclinical Models of Heart Failure. Circ Heart Fail. 2021;14:e007684. PMID: 33346675
- Chu Y, et al. β-hydroxybutyrate administered at reperfusion reduces infarct size and preserves
cardiac function. J Mol Cell Cardiol. 2024;186:1-12. PMID: 37979443
- Gopalasingam N, et al. Stimulation of the Hydroxycarboxylic Acid Receptor 2 With the Ketone Body
3-Hydroxybutyrate and Niacin in Patients With Chronic Heart Failure. JAHA. 2023;12:e029212.
PMID: 37301762
- Berg-Hansen K, et al. Beneficial Effects of Ketone Ester in Patients With Cardiogenic Shock.
JACC Heart Fail. 2023;11:1337-1347. PMID: 37452805
- Berg-Hansen K, et al. Cardiovascular Effects of Oral Ketone Ester Treatment in Patients With Heart
Failure With Reduced Ejection Fraction. Circulation. 2024;149:1763-1773. PMID: 38533643
- Gopalasingam N, et al. Randomized Crossover Trial of 2-Week Ketone Ester Treatment in Patients With
Type 2 Diabetes and Heart Failure With Preserved Ejection Fraction. Circulation.
2024;150:1061-1073. PMID: 39162035
- Guldbrandsen H, et al. Cardiovascular and Metabolic Effects of Modulating Circulating Ketone Bodies
With 1,3-Butanediol in Patients With Heart Failure With Reduced Ejection Fraction. JAHA.
2025. PMID: 39719429
- Nielsen R, et al. Hemodynamic Effects of Ketone Bodies in Patients With Pulmonary Hypertension.
JAHA. 2023;12:e028232. PMID: 37183871
- Ho KL, et al. Myocardial ketone body oxidation contributes to empagliflozin-induced improvements in
cardiac contractility. Circulation. 2025. PMID: 40069113
The Ask
Strategic partner for HFpEF Phase 2b trial (~$25M)
6 completed RCTs establish human proof-of-concept. Next step: registration-quality efficacy trial.
joel@senoviabiosciences.com